Evidence of Success
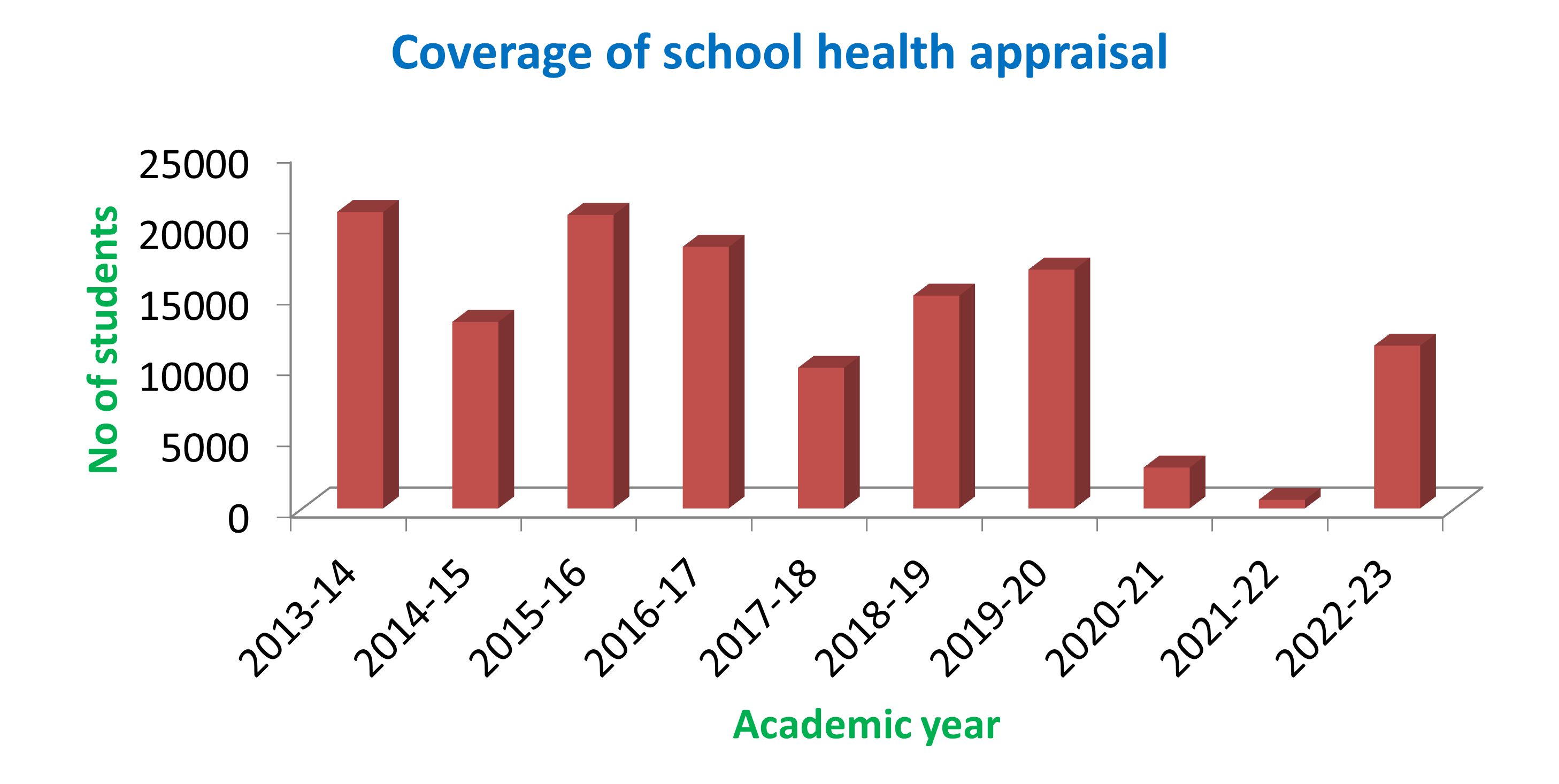
Graph showing Coverage of school health programme in last five years
The school health programme has been a successful event since years. This is evidenced by sustained reduction in the preventable morbidities among school children. There is also improvement in the reporting rates of illnesses among the school children this is due to improved awareness regarding the illnesses. The acceptability of health appraisal has enormously improved over years which is evidenced by increasing demand being posed by the school authorities to undertake the exercise. Six articles on different dimensions of school health programme are published in peer reviewed journals. As a result of Swachh Bharat- Swachh school abhiyana, most of the schools have been declared as plastic free zones. The recommendations pertaining to healthful school environments have helped the school authorities make infrastructural modifications in the schools.
Flow chart of activities

Evidence of Success
A total of 37646 people across 22 villages in four districts are covered under the project so far. 1827 health awareness sessions, involving seventeen village level link workers and 12 supervisory staff from the were conducted. 6511 people underwent health check up and received treatment in 33 health camps across these villages. 1752 school children across seven schools have also received health education through 97 sessions. The knowledge of villagers about the causes, symptoms, prevention and treatment of the diseases like hypertension, diabetes, anemia and MCH problems were found to be poor in the base line survey (survey conducted before educational interventions), the terminal survey results after series of health education activities have shown that there were significant improvement in the knowledge related to above mentioned domains.
Assessment of qualitative factors like acceptability of the awareness activities, attendance to the sessions, satisfaction with services, cooperation with link workers, participation in health camps, seeking care for these ailments have also improved over a period of time. Feedback from link workers also suggest that they feel empowered by the project and are able to help their villagers with their knowledge obtained through the project.
Problems Encountered
- The project had to be implemented in Northern Part of Karnataka with it's administrative centre in Southern part of the state, Mysuru, which are situated almost 500 Kms apart. Thus it was difficult job to go there in- person and deliver the services by the team situated in the institution.
- The second challenge was to get in tune with the socio-cultural specificities of the target population, especially the language, familial and community relationships, social structure, communication etc.
- Gaining the confidence of the target population was the third important challenge. As the implementing institution is far away from the service zone and people were not aware of the community extension activities offered by our organization. This has raised the issue of credibility and acceptance of the project related activities and services.
- Fourth challenge was mobilizing the people to accept the awareness messages and adapt them for positive behaviour change.
Resources required
Reaching larger section of population need more number of link workers and supervisors, but in rural areas getting such people is a difficult task. Sometimes link workers face difficulty in answering the queries raised by the villagers on these thrust areas, thus we are thinking of technology driven awareness sessions through interactive E gadgets, and telemedicine approaches. We are working towards locally tailored health education materials adapting the local language and culture which need larger intellectual inputs from experts and community. There is also a demand for increasing the number of health check up camps and increasing advocacy for the community mobilization.